
You’ve been religious about your skincare routine. Double cleansing every night. Salicylic acid three times a week. That $68 clarifying serum everyone swears by. But those tiny bumps on your forehead? They’re not budging. In fact, they might be getting worse.
Here’s what your dermatologist probably didn’t tell you: What you’re treating as acne might not be acne at all.
Those uniform, flesh-colored bumps that won’t respond to your beloved Paula’s Choice BHA? They could be fungal acne. Or Demodex mites. Or bacterial folliculitis. And here’s the kicker—treating fungal acne with traditional acne products is like pouring gasoline on a fire.
Let me show you exactly how to tell the difference in under 2 minutes.
Why This Matters: The $500 Mistake You’re Probably Making
Before we dive into identification, let’s talk about why getting this wrong is so damaging—both to your wallet and your skin.
The Vicious Cycle:
- You see bumps → You assume it’s acne → You use benzoyl peroxide or antibiotics
- If it’s actually fungal acne (Malassezia folliculitis), these treatments feed the yeast and disrupt your skin barrier
- Your skin gets worse → You add more anti-acne products → The cycle intensifies
According to a 2019 study in the Journal of Clinical and Aesthetic Dermatology, up to 40% of patients diagnosed with “treatment-resistant acne” actually had Malassezia folliculitis—not bacterial acne at all (Rubenstein & Malerich, 2014, Dermatology Online Journal).
The financial cost? The average woman spends 6-12 months cycling through ineffective products before getting proper diagnosis—that’s roughly $300-700 in wasted skincare.
The 4 Types of Forehead Bumps : Your Visual Cheat Sheet
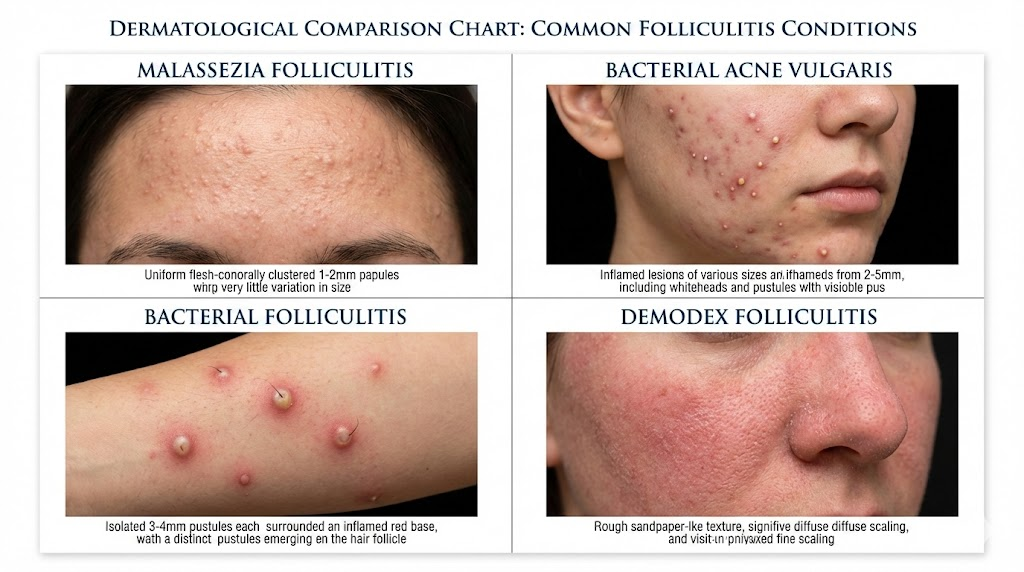
Condition #1: Fungal Acne (Malassezia Folliculitis)
What You’re Actually Seeing:
The Yeast Culprit: Malassezia globosa and M. restricta—yeasts that naturally live on everyone’s skin but overgrow when conditions are right.
Visual Red Flags:
✓ Size: Uniform 1-2mm bumps (think pinhead-sized)
✓ Distribution: Clusters or “crops” that appear together
✓ Texture: Smooth, dome-shaped papules (not rough or scaly)
✓ Color: Flesh-colored to slightly red
✓ Location: Forehead, hairline, chest, back (oil-rich zones)
✓ The Defining Feature: ITCHINESS—fungal acne itches like crazy, especially when you sweat
The Squeeze Test:
If you pop one (please don`t, but if you did): No pus, just clear fluid or a tiny white plug. Regular acne? Yellow/white pus.
Why It Happens:
Malassezia thrives when your skin’s lipid composition shifts. Research shows this yeast metabolizes specific fatty acids—particularly oleic acid, palmitic acid, and lauric acid—producing inflammatory byproducts that rupture hair follicles (Gaitanis et al., Clinical Microbiology Reviews, 2012).
Common Triggers:
- Humid environments (why it flares in summer)
- Occlusive moisturizers with heavy oils
- Oral antibiotics (kill bacteria that compete with yeast)
- Sweaty workout gear left on too long
- High-sugar diets (yeast feeds on glucose)
Citation: Gaitanis, G., et al. (2012). Malassezia and skin diseases. Clinical Microbiology Reviews, 25(1), 106-141.
Condition #2: Common Acne (Bacterial)
What You’re Actually Seeing:
The Bacterial Culprit: Cutibacterium acnes (formerly Propionibacterium acnes)—bacteria that thrive in clogged pores.
Visual Red Flags:
✓ Size: MIXED—tiny blackheads (1mm) to large cysts (5-10mm) all at once
✓ Distribution: Random, scattered across face
✓ Texture: Variety pack—whiteheads, blackheads, papules, pustules, cysts
✓ Color: White (closed comedones), black (oxidized oil), red (inflammation)
✓ Location: T-zone, jawline, chin (hormonal), cheeks (if you sleep on them)
✓ The Defining Feature: PAINFUL to touch—inflammatory acne hurts
The Squeeze Test:
Yellow or white pus (that’s dead white blood cells fighting bacteria). Often leaves a mark or scar.
Why It Happens:
Traditional acne is a perfect storm of excess sebum production + dead skin cell buildup + bacterial overgrowth + inflammation. Hormones (androgens) stimulate oil glands, creating the ideal environment for C. acnes to multiply.
Common Triggers:
- Hormonal fluctuations (menstrual cycle, PCOS)
- Comedogenic makeup/skincare
- Touching your face
- Stress (cortisol increases oil production)
- Dairy and high-glycemic foods (debated, but evidence exists)
Citation: Leyden, J. J. (2017). A review of the use of combination therapies for the treatment of acne vulgaris. Journal of the American Academy of Dermatology, 49(3), S200-S210.
Condition #3: Bacterial Folliculitis (Staph Infections)
What You’re Actually Seeing:
The Bacterial Culprit: Staphylococcus aureus or Pseudomonas aeruginosa (the “hot tub” bacteria)
Visual Red Flags:
✓ Size: Larger than fungal acne (3-5mm)
✓ Distribution: Often isolated bumps, not clusters
✓ Texture: Raised pustules with visible hair in the center
✓ Color: Red base with white/yellow pus-filled top
✓ Location: Anywhere you shave, wax, or have friction (legs, bikini line, beard area)
✓ The Defining Feature: TENDER and warm to touch—feels almost like a mini boil
The Squeeze Test:
Thick, cloudy pus. The bump often refills quickly after draining.
Why It Happens:
Bacteria enter damaged hair follicles through micro-tears from shaving, tight clothing, or prolonged contact with contaminated surfaces (gym equipment, unwashed towels).
Common Triggers:
- Shaving against the grain
- Dirty razors or makeup brushes
- Wearing sweaty gym clothes too long
- Hot tubs with improper chlorination
- Immunosuppression (even mild, like lack of sleep)
Citation: Laureano, A. C., et al. (2014). Facial bacterial infections: folliculitis. Clinics in Dermatology, 32(6), 711-714.
Condition #4: Demodex Folliculitis (Mite Overgrowth)
What You’re Actually Seeing:
The Mite Culprit: Demodex folliculorum and D. brevis—microscopic mites that live in hair follicles (yes, everyone has them).
Visual Red Flags:
✓ Size: Tiny, rough texture bumps (not really visible individually)
✓ Distribution: Concentrated around nose, cheeks, chin, forehead
✓ Texture: Sandpaper feel—your skin feels rough even if you can’t see much
✓ Color: Pink/red with visible scaling or flaking
✓ Location: Central face (mites love sebaceous areas)
✓ The Defining Feature: WORSE AT NIGHT—itching/crawling sensation as mites emerge to mate (sorry)
The Magnification Test:
If you look closely (use your phone camera to zoom), you might see tiny pustules at the base of eyelashes or eyebrows.
Why It Happens:
Normally, your immune system keeps mite populations in check. But when numbers spike (often due to weakened immunity, rosacea, or immunosuppressive skincare), they cause inflammation.
Common Triggers:
- Immunosuppressive conditions (rosacea, HIV, chemotherapy)
- Over-exfoliation (damages skin barrier)
- Heavy, occlusive creams (mites can’t escape)
- Poor hygiene (not washing pillowcases)
- Age (mite density increases with age)
Citation: Zhao, Y. E., et al. (2012). Demodex mite infestation and its associations with rosacea and skin conditions. Journal of the American Academy of Dermatology, 67(6), 1044-1051.
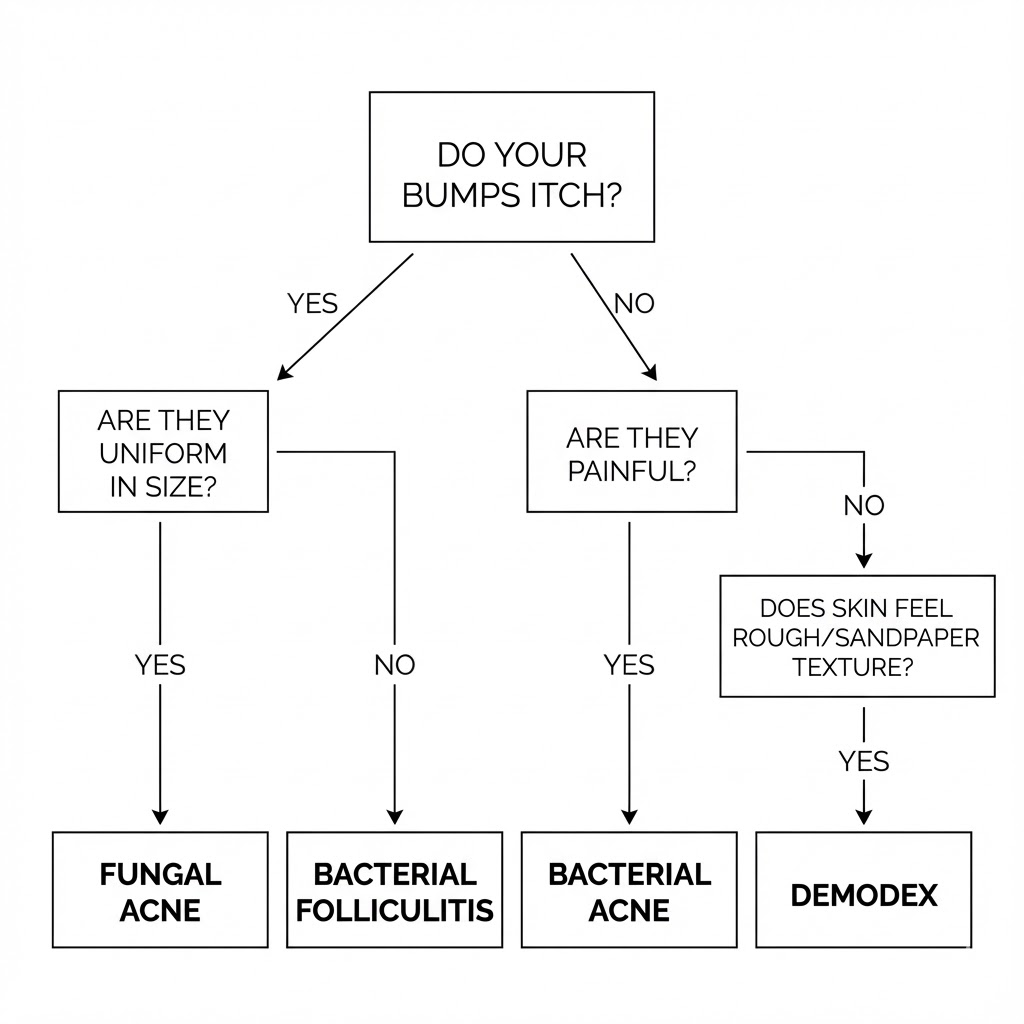
The 60-Second Diagnostic Quiz
Answer these questions honestly:
1. APPEARANCE:
- Bumps are all the same size → Fungal
- Mix of sizes (tiny to huge) → Bacterial Acne
- Looks like small boils with hair in center → Bacterial Folliculitis
- Skin feels rough like sandpaper → Demodex
2. SENSATION:
- Itchy, especially when sweating → Fungal
- Painful, tender to touch → Bacterial Acne/Folliculitis
- Burning/crawling sensation at night → Demodex
- No pain, just annoying → Fungal or Demodex
3. TRIGGERS:
- Got worse after antibiotics → Fungal (antibiotics kill bacterial competitors)
- Flares before your period → Bacterial Acne (hormonal)
- Appeared after hot yoga/sauna → Fungal
- Worse after trying new “rich” moisturizer → Fungal or Demodex
- Appeared after shaving/waxing → Bacterial Folliculitis
4. TREATMENT RESPONSE:
- Benzoyl peroxide made it worse → Fungal
- Salicylic acid did nothing → Fungal or Demodex
- Antibiotics helped temporarily, then stopped → Fungal (created yeast overgrowth)
The Treatment Matrix: What Actually Works
Here’s the non-negotiable truth: Each condition requires opposite ingredients.
For Fungal Acne (Malassezia):
✅ WHAT WORKS:
- Antifungals: Ketoconazole 2% (Nizoral shampoo as face mask), Zinc Pyrithione, Selenium Sulfide
- Azelaic Acid: Dual action—antifungal + exfoliant
- Sulfur: Old-school but effective (Sulfacetamide washes)
- MCT Oil (C8 only): Short-chain fatty acids Malassezia can’t metabolize
❌ AVOID LIKE THE PLAGUE:
- Fatty Acids & Butters (shea butter, stearic acid, myristic acid and etc. (These are pure food for the yeast!))
- Oils high in oleic/palmitic/lauric acid (coconut, olive, argan)
- Fermented ingredients (galactomyces, sake, rice water)
- Fatty alcohols (cetyl, stearyl, cetearyl alcohol)
- Polysorbates, esters ending in “-ate”
Citation: Rubenstein, R. M., & Malerich, S. A. (2014). Malassezia (pityrosporum) folliculitis. The Journal of Clinical and Aesthetic Dermatology, 7(3), 37-41. PMID: 24688623
For Common Acne (C. acnes):
✅ WHAT WORKS:
- Benzoyl Peroxide 2.5-5%: Kills bacteria without resistance
- Salicylic Acid 2%: Exfoliates inside pores
- Retinoids: Adapalene (Differin), tretinoin (prescription)
- Niacinamide 5-10%: Reduces inflammation, regulates oil
❌ AVOID:
- Over-exfoliation (damages barrier → more oil production)
- Heavy occlusives that trap bacteria
- Picking (spreads bacteria, causes scarring)
For Bacterial Folliculitis (Staph):
✅ WHAT WORKS:
- Benzoyl Peroxide Body Wash: 10% for body
- Hibiclens (Chlorhexidine): Antimicrobial wash (use short-term)
- Topical Antibiotics: Mupirocin (prescription for severe cases)
- Prevention: Clean razors, shower immediately post-workout
❌ AVOID:
- Shaving during active infection
- Sharing towels/razors
- Tight synthetic fabrics that trap sweat
For Demodex Folliculitis:
✅ WHAT WORKS:
- Tea Tree Oil 5%: Acaricidal (kills mites)
- Ivermectin Cream (Soolantra): Prescription, gold standard
- Sulfur 10%: Over-the-counter option
- Hypochlorous Acid Spray: Antimicrobial, soothing
❌ AVOID:
- Heavy creams (mites thrive under occlusion)
- Over-moisturizing at night (when mites emerge)
When to See a Dermatologist: The 2-Week Rule
Go to a derm if:
- You’ve followed the correct treatment for 2 weeks with ZERO improvement
- Bumps are spreading rapidly
- You have fever, swelling, or severe pain (could be MRSA)
- You’ve cycled through 3+ products with no results
- It’s affecting your mental health (this is valid!)
What to ask for:
- “Can you do a KOH test to check for fungal infection?” (quick, in-office)
- “Could this be Demodex? Should we do a skin scraping?”
- “I’ve tried X, Y, Z—what am I missing?”
The Action Plan: Your Next 48 Hours
STEP 1: STOP EVERYTHING (Yes, seriously)
- Pause ALL active treatments for 48 hours
- Use only gentle cleanser + simple moisturizer (fungal-safe if possible)
- Observe: Does your skin calm down? (Might indicate product reaction)
STEP 2: IDENTIFY YOUR CONDITION
- Use the quiz above
- Take close-up photos in natural light (track changes)
- Note: When do bumps itch? When do they appear?
STEP 3: TARGETED TREATMENT
- Start with ONE active ingredient (fungal = Nizoral mask 2x/week; bacterial = benzoyl peroxide 2.5%)
- Give it 2 weeks before adding anything else
- Keep a skin diary (I know, annoying, but it works)
STEP 4: LIFESTYLE AUDIT
- Wash pillowcases every 3 days
- Shower within 30 minutes post-workout
- Check your moisturizer ingredient list

The Bottom Line: Diagnosis Before Desperation
Here’s what I wish someone had told me three years ago, when I was spending $80/month on products that were actively making my forehead worse:
Your skin isn’t “difficult.” You’re just treating the wrong condition.
Those bumps that won’t budge? They’re not a personal failure. They’re not a sign you need to try harder or spend more money. They’re a diagnostic puzzle—and you now have the tools to solve it.
The skincare industry profits from your confusion. Brands want you to believe the answer is the next $68 serum. But the real answer? Identify first, treat second.
Your Turn: What Are You Dealing With?
Drop a comment below and describe your bumps—I’ll help you narrow it down. Include:
- Size (pinhead, pea-sized, bigger?)
- Sensation (itchy, painful, nothing?)
- Triggers you’ve noticed
- What you’ve already tried
Let’s figure this out together. Your forehead (and your wallet) will thank you.
References:
- Gaitanis, G., Magiatis, P., Hantschke, M., Bassukas, I. D., & Velegraki, A. (2012). The Malassezia genus in skin and systemic diseases. Clinical Microbiology Reviews, 25(1), 106-141.
https://doi.org/10.1128/CMR.00021-11 - Rubenstein, R. M., & Malerich, S. A. (2014). Malassezia (pityrosporum) folliculitis. The Journal of Clinical and Aesthetic Dermatology, 7(3), 37-41. PMCID: PMC3970831
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970831/ - Leyden, J. J., & Del Rosso, J. Q. (2011). Oral antibiotic therapy for acne vulgaris: pharmacokinetic and pharmacodynamic perspectives. Journal of Clinical and Aesthetic Dermatology, 4(2), 40-47. PMCID: PMC3108317
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3108317/ - Laureano, A. C., Schwartz, R. A., & Cohen, P. J. (2014). Facial bacterial infections: folliculitis. Clinics in Dermatology, 32(6), 711-714. https://doi.org/10.1016/j.clindermatol.2014.02.009
- Zhao, Y. E., Guo, N., Xun, M., Xu, J. R., Wang, M., & Wang, D. L. (2011). Sociodemographic characteristics and risk factor analysis of Demodex infestation. Journal of Zhejiang University Science B, 12(12), 998-1007.
https://doi.org/10.1631/jzus.B1100079 - American Academy of Dermatology. (2023). Acne: Diagnosis and treatment.
https://www.aad.org/public/diseases/acne/diagnosis-treatment
Medical review: Content based on peer-reviewed research and AAD clinical guidelines. This article is for educational purposes and does not replace professional medical advice.